

In collaboration with

Exercise for trans young people: what 20 stakeholders told us, and what it means for practice
New research lead by Dr Felicity Austin (UWA), and co-authors from the MHEX Team. Published July 2026 by Psychology of Sport + Exercise.
Trans young people are not refusing to exercise, they are being pushed out of exercise and sport spaces. That is the thread running through our new paper, just accepted in Psychology of Sport & Exercise, which brings together the voices of 20 stakeholders across Australia to ask a simple but impactful questions: how should specialist paediatric gender diversity services and exercise professionals support trans adolescents to be physically active in ways that are safe, affirming, and sustainable?
This post is for exercise professionals, exercise physiologists, allied health clinicians, and program designers working at the intersection of physical activity, mental health, and gender-affirming care. The paper itself is open access, and linked at the bottom of the page.
Why this question matters
Roughly 3.3% of high-school-aged Australians identify as trans or gender diverse. They report significantly lower levels of regular physical activity than their cisgender peers (Austin et al 2024), and the Trans Pathways data tell us that 81% of trans young people in Australia want to exercise more but feel unable to. They also experience markedly higher rates of depression, anxiety, self-harm, and suicidality, much of which is driven by minority stress and exclusion rather than by gender itself.
Exercise is a known support for mood regulation, social connection, bone and metabolic health, and body congruence during gender-affirming medical care. Yet exercise professionals are not currently embedded in standard paediatric gender diversity services in Australia. The gap is large, and the people most affected by it are the people least likely to be able to walk into a gym or sports club and feel safe enough to stay.
Most prior qualitative work on trans young people and movement has focused on community sport, school physical education, or adult populations. Almost none has looked at how trans adolescents experience exercise inside the clinical pathways that already see them. That is the gap our team set out to fill as part of Dr Felicity Austin’s PhD.
What we did
We used reflexive thematic analysis grounded in interpretivism and informed by intersectionality theory. Twenty stakeholders took part: 6 trans young people, 2 parents and carers, and 12 healthcare providers including general physicians, psychiatrists, psychologists, speech therapists, social workers, exercise physiologists, and gender diversity research staff.
Recruitment was through specialist paediatric gender diversity service networks across Australia and aligned social media channels. Lived-experience participants were interviewed individually; healthcare providers were interviewed in small focus groups. Interviews averaged around 50 minutes. The interview guide was reviewed by the GENTLE Consumer Advisory Group at Perth Children’s Hospital before use.
Analysis was iterative, with critical friend discussions across six meetings over four months. The team brought reflexive practice to the work, which mattered: most of us are cisgender, allied health, and clinically connected to trans care. We built that positioning into how the analysis was interpreted, rather than pretending it was not there.
What we found
Four interrelated themes were generated: navigating intersectionality in adolescence; the binary nature of community sport and physical activity spaces; external pressures and societal marginalisation shaping participation; and inclusive exercise as a reimagined social practice.
Below are the practitioner-facing takeaways that the data point to most clearly.
1. Inclusion is structural, not cosmetic
Trans young people described running constant risk assessments before stepping into sport or exercise spaces: Which change room? Which uniform? Which bathers? Whether their binder would be visible? Whether someone might say something?
These are not personal preferences, they are the binary architecture of community sport and school PE doing the gatekeeping and a flag on the wall does not undo that.
For practice, this means auditing the structural defaults of your exercise services and spaces before the inclusion messaging: intake forms (do they collect gender, pronouns, and name in use), group allocation logic, change facilities, dress codes, and whether participants can move between groups without administrative friction.
2. Neurodivergence and gender diversity overlap, and the interaction matters
Around 7.8% of adolescents referred to gender clinics also have Autism or ADHD. Participants described how sensory load, executive function demands, social communication in team sport, and routine disruption interact with dysphoria, hormone treatment, and minority stress. A program that adjusts for gender alone still fails neurodivergent trans young people.
Practical adjustments that participants and clinicians flagged: predictable session structure communicated in advance, sensory-aware environments (lighting, noise, equipment choices), autonomy over activity choice, consistent staffing, flexible clothing, and gradual skill progression. None of this is new, it is good exercise prescription applied with intent.
See more on the eating and exercise experiences of trans and gender-diverse people from Schweizer et al 2026 and some community summary sheets from the MHEX team
3. Gender-affirming medical care changes the function of exercise
Exercise was described as protective when paired with gender-affirming hormones, helping to manage body composition shifts, supporting bone health during puberty suppression, and building social confidence before discharge. It was also described as something young people leaned on while waiting for care, sometimes in restrictive or compulsive ways.
This is an argument for early integration of an exercise professional into the multidisciplinary team rather than late referral. It is also an argument against treating motivation as a reliable proxy for healthy engagement. Map exercise behaviours against treatment stage, waitlist position, and access to care.
4. Withdrawal happens before participation
Many of the avoidance patterns described were anticipatory rather than reactive. Young people had not necessarily had a bad experience at a specific gym. They had read enough media coverage of trans participation in sport to assume one was coming. One unwelcoming encounter often closed off a whole category of activity.
Importantly, silence reads as risk. If your service is inclusive, make that explicit on every surface participants encounter before they meet you: website copy, intake forms, signage, the language used in confirmation emails. Pre-empt the first session by walking through what to expect.
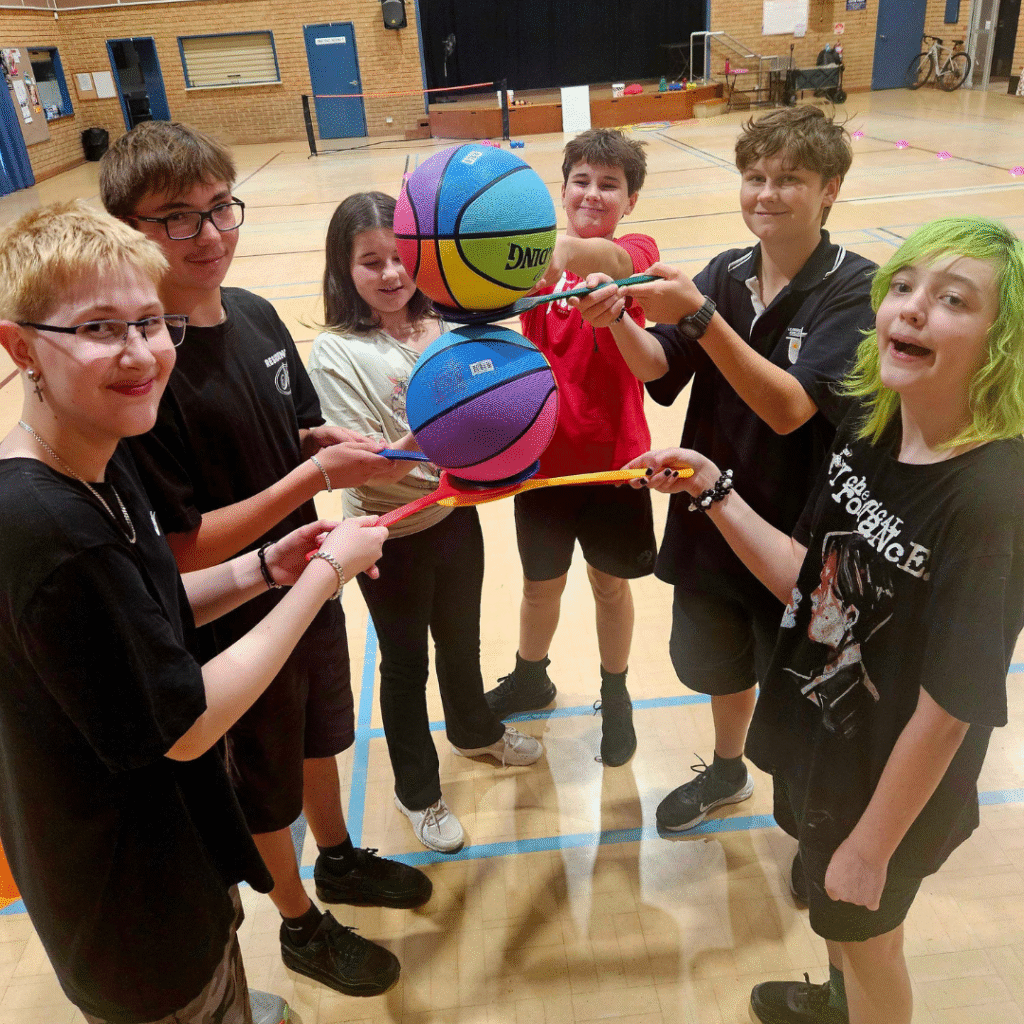
5. Peer connection is the primary mechanism, not a side benefit
Group settings with shared identity reduced the cognitive load of self-monitoring. Younger participants described learning about hormones, transition, and life logistics from older peers in the same room. That is not something a 1:1 exercise session can replicate.
Where service capacity allows, group programs that bring trans young people together in mixed-stage cohorts will likely outperform solo delivery for engagement and retention. This is also a useful funding argument for cohort-based delivery in hospital and community settings. Check out Thriving in Motion programs in action!
What it means for practice
If you are an exercise physiologist or allied health practitioner working with trans young people, the data point to a small set of moves that consistently come up across both lived-experience and clinician accounts.
- Audit the structural defaults of your service (intake, group allocation, facilities, uniforms) before refining your inclusion messaging.
- Build sensory-aware, predictable session design as the baseline, not an accommodation.
- Treat standard screening tools as a conversation opener (e.g., disordered eating); add binding history and body-goal questions.
- Embed exercise professionals into the multidisciplinary team early, not at discharge.
- Use group format with mixed-stage peers wherever capacity allows.
- Make inclusion explicit on every pre-session surface so silence does not get read as risk.
- Plan the bridge from hospital-based programs into community pathways (such as Thriving in Motion or other inclusive providers) before discharge, not at it.
These are also the design principles informing the next phase of work. Our team is leading a national rollout and evaluation of an exercise intervention developed from this research, embedded in specialist paediatric gender diversity services and bridged into community pathways. The clinical trial registration is ACTRN12625000351412, and it is part of a larger national collaboration in gender health research – ARCTYC.
Honest about the limits
Twenty stakeholders is a sample size sized for depth, not for breadth. The young people who took part were already engaged with specialist paediatric gender diversity services, were 18 or older at the time of interview, and most or all came from supportive families. Trans young people without supportive families, without service access, or outside metropolitan networks will likely have different and harder stories. Future work needs to bring those voices in, including via the qualitative arm of the upcoming trial with adolescents aged 12 to 17.
How to access the paper
Paper is available to everyone via journal, Psychology of Sport & Exercise: “Austin, F., Lin, A., Wright, K., Jackson, B., Simpson, A., & Furzer, B. (2026). Exercise Experiences of Adolescents Engaged with Gender Diversity Services: A Qualitative Approach. Psychology of Sport & Exercise.”
- Open access link: https://doi.org/10.1016/j.psychsport.2026.103148
- Funding: Australian Government Research Training Program Scholarship (FA).
- Linked clinical trial: ACTRN12625000351415
Talk to us
If you are working in exercise, allied health, or gender-affirming care and would like to connect with the MHEX research group, share your service-level experience, or discuss the rollout, get in touch via mhex@uwa.edu.au or follow us on Instagram (@mhexresearch) and LinkedIn (Mental Health + Exercise Research Group).
More MHEX News




The MHEX Team acknowledges all Aboriginal and Torres Strait Islander Traditional Custodians of Country and recognises their continuing connection to land, sea, culture and community. We pay our respects to Elders past, and present.
We are committed to embracing diversity and eliminating all forms of discrimination through education and inclusive communities. We welcome all people and are respectful of individual identities.