
MHEX Research
Exercise and Youth Mental Health Service Transitions: What a New Review Means for Practice
For many young people living with mental illness, one of the most vulnerable points in their care isn’t a diagnosis or a crisis, it a transition in care. A new narrative review led by PhD Candidate Ben Kramer and his team of researchers at the University of Western Australia (UWA), UNSW, The Kids Research Institute Australia, and Fremantle Hospital Mental Health Service examines what happens when youth move from child and adolescent mental health services (CAMHS) into adult mental health services (MHS), and asks whether structured exercise could help keep them engaged in care through that shift. The review, led by exercise physiologist and UWA PhD candidate Ben Kramer, alongside A/Prof Kemi Wright, Prof Ben Jackson, Dr Aaron Simpson, and A/Prof Bonnie Furzer, was published in Mental Health and Physical Activity.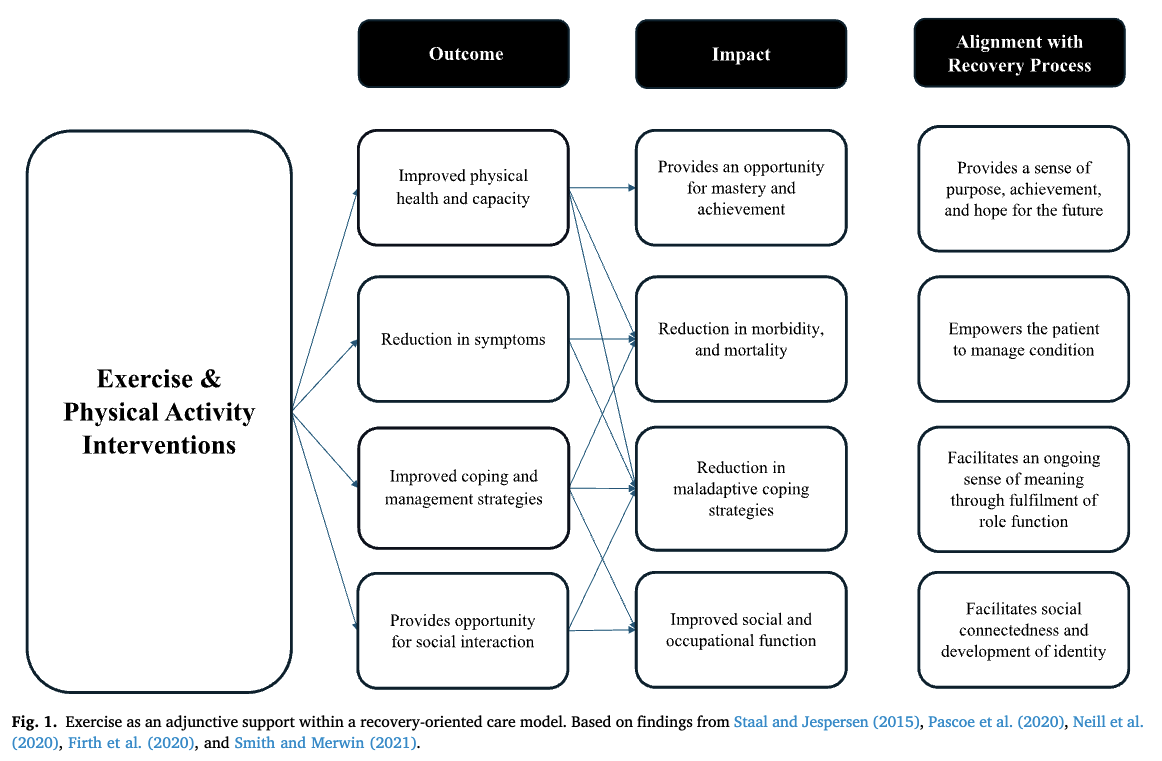
Why This Question Matters
Youth mental illness carries a heavy individual and societal cost. Late adolescence and early adulthood are when mental illness is most likely to first appear, and this period overlaps with major life changes including finishing school, entering the workforce, and building independence. For young people already managing a mental illness, this is also often when they are required to transition from CAMHS to youth or adult mental health services. The review outlines a consistent finding across the literature: this transition is a high-risk period for disengagement. Youth face personal barriers, such as new obligations and a loss of trusted clinician relationships, alongside organisational barriers including inconsistent referral practices and gaps in communication between services. Many describe a “culture shock” moving from the holistic, family-oriented approach typical of CAMHS to the more diagnostic, autonomy-driven model of adult MHS. Disengagement during this window is not a minor administrative issue. The review links it to increased rates of hospitalisation, mental health-related emergency department presentations, and mortality, underscoring why closing this gap matters for practitioners and services alike.What Was Done
This was a narrative review, drawing together three intersecting bodies of literature: youth experiences of transition between child and adult mental health services, recovery-oriented models of care, and structured exercise as an adjunctive mental health intervention. The authors searched Ovid (Embase, PsycINFO, MEDLINE) and Scopus, supplemented by grey literature and hand-searching of reference lists, with findings synthesised thematically rather than through a systematic or exhaustive process.What Was Found
The review makes the case that structured exercise sits at a useful intersection of care and recovery. It aligns closely with the five pillars of recovery-oriented care identified in the mental health literature: connectedness, hope and optimism, identity, meaning, and empowerment. It also addresses developmental priorities that adult mental health services are often not designed to meet, including identity formation, social connectedness, and vocational or educational engagement. Across existing youth exercise intervention studies, the authors found consistently high rates of adherence, acceptability, and participant satisfaction, alongside low dropout, even though no study to date has specifically examined exercise as a tool for supporting the transition between services. This is an important gap, as the feasibility evidence is strong, but the transition-specific evidence does not yet exist.Key finding: Structured exercise addresses the known drivers of youth disengagement, services that feel deficit-focused, lost provider relationships, and a lack of youth-specific support, making it a promising, low-barrier addition to transitional care.
What It Means for Practice
For exercise physiologists, psychologists, and mental health clinicians working with young people, the review offers a practical framing: exercise does not need to replace clinical care to be valuable during a transition. It can be embedded within or alongside existing services without requiring a fundamental redesign of care pathways.- Consider where a structured, needs-supportive exercise offering could sit within your service’s transition planning, particularly for young people at risk of disengagement.
- Frame exercise participation around connectedness, mastery, and identity, rather than symptom reduction alone, in line with recovery-oriented principles.
- Look for opportunities to maintain a consistent point of contact, such as an exercise physiologist, across the transition, where clinical relationships might otherwise be lost.
Full Citation
Kramer, B., Wright, K., Jackson, B., Simpson, A., & Furzer, B. (2026). Exercise as a novel treatment to improve engagement with mental health services in youth with clinical mental illness: Review and recommendations. Mental Health and Physical Activity, 31, 100801.
Take Part in Our Current Research
This review is also the foundation for a qualitative study now underway at UWA, exploring the experiences of young people, parents, and clinicians navigating this exact transition, and whether a needs-supportive exercise service could help.Youth Experiences of Service Transition Within Mental Health Services, and the Role of Exercise as a Support
We would love to hear from and collaborate with:
- Young people (15–25 years) who have transitioned out of, or been discharged from, Child and Adolescent Mental Health Services in the last 4 years
- Parents of young people who have transitioned out of Child and Adolescent Mental Health Services over the last 4 years
- Youth and community healthcare and support workers experienced in the treatment and management of young people with mental illness
Participation involves 1–2 interviews, 3–6 months apart (2 x 60 minutes) at UWA, online, or a location that suits you, or an online response option instead of interviews for young people with lived experience.
For more information, contact Ben Kramer (PhD Candidate) or Bonnie Furzer (Chief Investigator). Approved by the UWA Human Research Ethics Committee (2022/ET000948).